


Pandemic Excess Deaths -Cause and Significance

Very interesting post by Brian Mowrey as the Pandemic staggers to the finish line, to be quickly forgotten or repeated.
I was going to leave a comment on Brians stack but it turned out too long for a comment but perfect for its own post.
Brian covers a lot of ground in his post, some of which I agree with. I will focus more on what I don’t agree with. I suggest you read his post , before continuing but if you don’t, the below passage will start us off.
If I understand his post correctly Brian argued the virus is responsible for many of the Excess Deaths, the Vaccines may be at least somewhat effective, and in any event the Excess Deaths are not that significant so lets move on. I am paraphrasing, these are not direct quotes.
I might quibble with “many”, not as much with “at least somewhat”, but I don’t agree to downplay the “significance”
His larger point which I agree with is regardless of what is most responsible , is we should still have our freedoms, including freedom from being experimented on, even if it means more deaths in the community.
My apologies if I misunderstood anything. Read and decide for yourself

Lets start with this
Of the US, I would argue that more would have died without the transfections, given first that our comorbidities outstrip what prevails in Southern Africa and Asia, and second that most Americans did not get infected until after injection (since thanks either to the lockdowns or to deficiencies in the virus that had to be worked out via mutation, few people were actually infected in 2020 outside of nursing homes in New York and New Jersey).
I don’t agree the vaccines had a net positive impact on reducing total deaths. The data is clear. More people died after vaccinations than in 2020, even sans Lockdowns. Proof one way or the other is lacking, so we have to use our best judgement.
And most people did get their first infection after they were vaccinated. Why would that be? Perhaps the vaccines did something to compromise people natural immunity. Perhaps reliance on serum antibodies that wane rapidly to protect against a respiratory virus that infects via your mucosa is a bad idea. Perhaps a massive vaccination campaign in the midst of a pandemic drives the virus to mutate and escape the immunity of the vaccinated. Perhaps repeated boosting to combat the new variants creates immune exhaustion allowing repeated infection and more severe disease!
I wont discuss the immunology here though, there are too many other aspects I wish to cover
While South Africa is a very young population (median age 27.6) and not heavily vaxxed, there was significant uptake (35% fully vaxxed, about 20 million people). It also has more poverty and a high HIV prevalence that would counteract their youth and lack of obesity. Also South Africa was a hard lockdown country starting from early on in the Pandemic which no doubt contributed to excess deaths, especially given their poverty levels
Brian shows a chart which has East Asia having few Excess Deaths
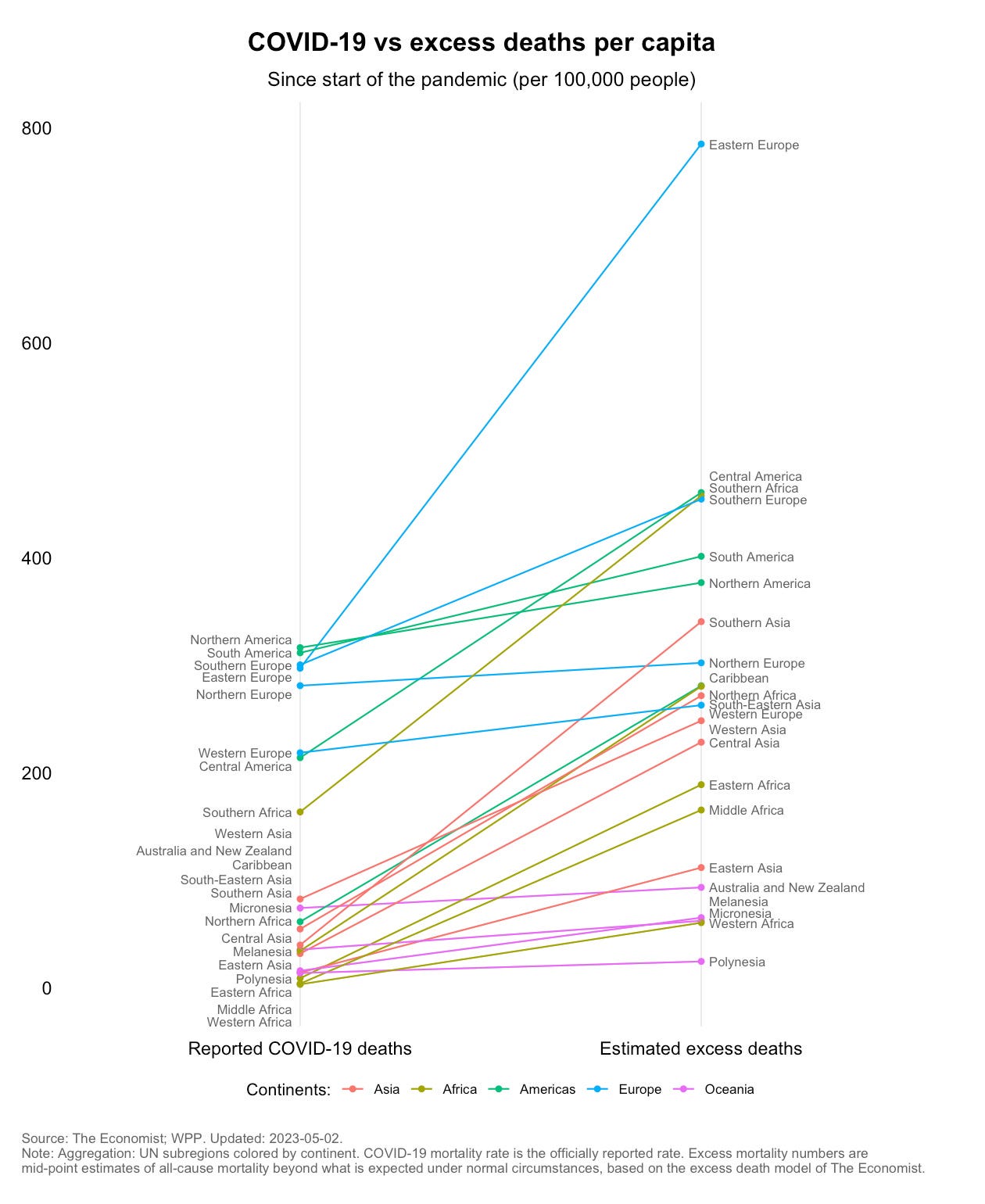
However, East Asia is possibly skewed by Chinas numbers which are not to be believed as they are either lies or are based on calculations and treatment not used by the rest of the world. Taiwan is an East Asian country and if you plot their data its much higher than the East Asia line (100 per 100,000 pop Covid, 200 per 100,000 Excess)
It strikes me that the US was far more efficient in classifying Excess Deaths as COVID (over 70% of Excess classified as COVID) than Asia and South Africa (30-50% of Excess Deaths classified as COVID), but this does not mean the US and West Europe were correct and Asia and South Africa were not. It is likely the financial incentives to classify deaths as COVID were greater in the West
Here is the latest Excess Deaths for East Asian countries scaled to make it hard to read. They don’t seem to have Chinas excess deaths for some reason

Hardly any deaths before the vaccinations began and these excess deaths accelerated as boosters rolled out
Brian also shows another chart of US Excess Deaths

Note the sharpest slopes: April, 2020; December, 2020; August, 2021; January, 2022.
I would point out April 2020 was when the novel virus began spreading albeit in a limited geographical area, December 2020 was when the vaccines rolled out in US, August 2021 was around when boosters and mandate campaign took off, and January 2022 was when a new virus began (Omicron).
There is reason to consider Omicron a separate virus which may also have a lab origin, but further elaboration is beyond the scope of this post. In any event, Omicron acted as a defacto self spreading booster shot.
Next up:
Significance of Excess Deaths
If we are all, in our individual connections, members of a village of 1,000, SARS-CoV-2 was never capable of being more than a minor tragedy, akin to a single house fire.
Almost 2 million dead Americans is some house fire, although to be fair I think he means Sars-Cov-2 alone. Sars-Cov-2 may have killed as few 300,000 without all the harmful protocols, restrictions on repurposed drugs, lockdowns and vaccines, and thus the analogy of a house fire in a population of 1000 is apt.
“Alright, but Australia has only racked up ~.8 excess deaths per 1,000 in all this time, vs. the USA’s 4. And 21,000 total excess deaths, as a high estimate, in a country of 26 million, just isn’t a lot.”
This is just 1 + years data unlike 3 + years in US. If you consider 10 in 1000 die ever year in a normal year 1 extra deaths is a lot, especially when prolonged over 3 consecutive years as in the US. And especially if you consider the survivors (of lockdowns, Covid or Jabs) who may be damaged and needing financial help or medical care as a result of their own illness or due to the loss of a spouse, parent or child.
There is also a possibility there will be a negative impact on life expectancy on the jabbed or COVID recovered, but we will not see any evidence of this for years, if it indeed occurs. This is just speculation, but if it occurs that house fire might be likened to Ground Zero after 9/11 which smoldered for many weeks releasing toxic gasses to detriment of the health and life expectancy of residents. They were assured the air was safe.
A major beneficiary of course is the Malthusians among us, and Social Security, Medicare and Pension Funds
Back to the main point. What is most responsible for Excess Deaths. I think we can agree that Lockdowns, COVID and the Jabs all contributed to some degree. Many of those excess deaths were subjected to all 3. The jabs might have delayed some COVID deaths for a few months (March-May) in 2021, so thats the limit of my agreement with “somewhat effective”.
I think we may all agree many of the COVID deaths were not actually deaths from COVID but were deaths for other reasons. This number may be as high as 25-50% of all COVID designated deaths. One might argue the extent but most will agree COVID deaths were overstated due to various financial incentives.
Many of those who died of COVID may well have been prevented if not for the harmful COVID treatment protocols pushed by the NIH , which included limiting use of repurposed drugs. Dr Kory suggested 80% could have been prevented. 25-50% seems more conservative but good luck proving any of these numbers.
So out of every 100 COVID deaths maybe only 50-75 were COVID deaths and only 25-50 of those needed to die of COVID
So while I don’t argue the virus can kill, I think its likely that many COVID deaths had more to do with the treatment protocols and denial of drugs that might have worked.
I am convinced that if we treated Covid like we did any other respiratory virus , ignoring it and letting Doctors treat patients without interference there would be relatively few excess deaths.
This Israeli Doctor (Prof. Udi Qimron, the Department of Clinical Microbiology and Immunology at Tel Aviv University.) seems to agree
"'If we had not been told that there was an epidemic in the country, you would not have known there was such an epidemic and you would not have done anything about it”
http://www.israelnationalnews.com/News/News.aspx/285341
There are a lot of variables and you can make a case for any of these VLCP (Vaccines, Lockdowns, COVID, Protocols) or any combination thereof being responsible
Presenting Taiwan As Evidence
Taiwan is rarely mentioned, maybe because data is a bit harder to get but IMO Taiwan helps us see through the smoke. It is the only country that had no Lockdowns AND had no Domestic Covid spread until Vaccinations began
Like Australia (slightly smaller population but much higher population density) most of Taiwans excess and Covid deaths began with boosters in 2022 with 1.6 per 1000 populationexcess deaths in 2022-2023 . But Taiwan also had its first COVID Wave starting in May 2021 which contributed another 0.4 per 1000 population excess deaths through the rest of the year
Taiwan did follow the US lead in COVID treatments, and restricted the use of drugs like IVM. Having a centralized system due to their National Insurance Program there were few Pharmacies or Doctors who were dispensing IVM or treating patients with IVM , unlike in US. They did however liberally hand out Paxlovid in 2022.
COVID CFR dropped from about 4% in 2021 to 0.15-0.20 % in 2022. The vast difference is likely due to Omicron and the under testing in 2021 vs a massive test program in 2022 using home antigen test kits and self reporting to confirm cases. The latter may be closer to an IFR than CFR with 99.5% of cases having mild or no symptoms.
IMO Taiwan is the smoking gun that the Vaccines were the main driver of Excess Deaths, with over 50% of Excess Deaths (and maybe 2/3) being Non-Covid, and its unlikely any COVID death was undiagnosed starting from May 2022 when over 95% of the COVID deaths occurred.
Later on I will present evidence, although fairly weak evidence given the paucity of data being provided, that up to 25-50% of the 2022 COVID deaths may have been with COVID and not from COVID
If only 25% of the COVID deaths reported were due to other reasons then almost 2/3 of EXCESS deaths were Non-Covid deaths
https://pete843.substack.com/p/taiwan-excess-death-update-no-end
FWIW charts for deaths and cases for Taiwan are still scrubbed on OWID. Its been consolidated with Chinas data. Taiwan is not reporting daily cases and deaths and seems the weekly reports have been delayed.
Anyways, while Taiwan does not have the obesity problem the US has (catching up though), it is an older population and has plenty of other morbidities, as is presumably Japan, both of which are highly vaxxed and dealing with significant Excess Deaths post vaccination campaigns. Both have high population densities so should have been susceptible to rapid spread of the virus in 2020.
In Taiwan, hundreds of thousands of their citizens were living (school or work) in China and other areas like US, Europe and UK that had bad 2020 COVID outbreaks. Many of them returned to Taiwan in the first quarter of 2020 when lockdowns started in these areas. Upon arrival there was no testing unless you had symptoms, so presumably some asymptomatic or pre-symptomatic COVID made its way into Taiwan, yet no outbreaks. Of course, given how little testing there was in the community at the time this would also explain the lack of cases, assuming the virus was not overly severe (except in the very frail and elderly who are regular victims of respiratory viruses and thus would be treated as flu).
There was in fact no excess deaths in 2020, and since there was no regular testing of COVID, so COVID treatment protocols were not followed. No denial of high dose steroids, no Remdesivir, no quick rush to place patients on Ventilators and give them drugs that suppressed respiration.
Only when vaccinations began did they ramp up testing and then have those who tested positive put on COVID Treatment protocols.
But even in 2021, after vaccinations began, COVID deaths amounted to only 10% of the total Excess Deaths. One reason for this is mostly only those incoming arrivals or those who presented at hospital with symptoms and their contacts were tested, so relatively few were put on these protocols.
Others will try to argue that masking and social distancing kept COVID at bay in 2020. But masks were not required for most of 2020 except on public transportation and hospitals. Indoor masking did not start until December 2020, and social distancing was a pipe dream in Taiwan until the first wave was declared in May 2021. Plus, we all know now the virus is airborne and masks are not very effective.
Anyways, my mind is open to the possibility of Long Covid contributing to excess deaths, but in the absence of good data or evidence, I think its likely that Long Covid is being used as cover for Vaccine Harm and its impact on excess deaths is being overstated
Undercounting Excess Deaths
Its likely Excess Deaths are underreported. If you take into account the pull forward effect, excess deaths in the US are probably closer to 2 million, over 6/1000 and a disproportionate number of excess deaths are working age adults, no doubt related to after effects of lockdowns and vaccinations
From Ethical Skeptic
https://twitter.com/EthicalSkeptic/status/1635606835532034050?s=20

So while you may see Total Deaths coming back to normal in US this is actually still elevated since with up to 2 million Excess Deaths over 3 years, expected deaths should be quite a bit below the 2016-2019 average used by CDC here

Indeed, if you look at it by age which I have no time to do..... wait a minute.....
I will do a quick and dirty calculation (compare to 2019) before I say something stupid
Total Death
Under 50
Total. *Excess. %
2019- 283,225
2020- 320,957. 37,732. 13.3%
2021- 363,620. 80,395. 28.4%
2022- 324,752. 41,527. 14.7%
*over 2019
50+.
Total. *Excess. %
2019- 2,571,613
2020- 3,069,082 497,461. 19.3%
2021- 3,108,139 536,526. 22.8%
2022- 2,953,295 381,683. 14.8%
*over 2019
Percent of Excess Deaths
Under 50. 50+
2020- 7.1. 92.9
2021- 13.0. 87.0
2022- 9.8. 90.2
Percent of Total Deaths
Under 50. 50+
2019- 9.9. 90.1
2020- 9.5. 90.5
2021- 10.5. 89.5
2022- 9.9. 90.1
There is uncertainty in my 2019 data. For some reason CDC showed Pre-Covid in different age groups than the COVID data set, instead of 50–64 it has 55-54 so I figured it safe to split it evenly. Like I said, quick and dirty
So basically, what I was about to say was about right. 2021 was a bad year for the under 50’s, but the VLCP was still mostly taking out the over 50’s. I wonder if anyone has calculated the savings for pension funds and social security?
Anyways, since I am talking COVID I will end by reposting part of my last Musings post.
One last note on Taiwan. COVID. At the end of March they began weekly reporting of COVID deaths and COVID cases with complications.
The latter, to the best that I can gather , are those which they have in the past reported as Moderate and Severe Cases. We have quite good data showing this to be about 0.5% of total cases. Keep this in mind as I go through the data.

The red is cumulative number of cases and percentage with mild or now symptoms. The rest is complicated cases with Moderate being 0.28% and severe 0.2%.
Note that the CFR has typically ranged from 0.15-0.20% which suggests a pretty high hospital mortality rate for those diagnosed as Moderate or Severe.
But first of all, let me break the news. They failed to report last weeks data, this being the first week of COVIDs favorite Month on Taiwan. No apparent explanation on their web site.
Here is the data from the weekly reports
Date. Deaths. Comp Cases Total Cases
2/24-3/23. 35/d. 119/d 9.6k/d
Note-here Complicated is 1.2% of total reported cases and not 0.5%. I think the reason is people had reduced self testing and reporting as the government began downplaying the disease, so for the estimated total cases I will use an average 0.85%
Deaths Comp Cases. Estimate
3/24-3/30. 25/d, 96 p/d. 11.3k/d
3/31-4/6. 15/d, 84 p/d. 9.9k/d
4/7-4/13. 17 /d 86 p/d. 10.1k/d
4/14-4/20. 13/d. 93/d. 10.9k/d
4/21-4/27. 13/d. 99/d. 11.6 k/d
Lets look at the CFR based on this
Date. CFR
2/24-3/23. * 0.36%
*likely high due to underreporting cases in this period
3/24-3/30. 0.22%
3/31-4/6. 0.15%
4/7-4/13. 0.17%
4/14-4/20. 0.12%
4/21-4/27. 0.11%
As you can see the trend is downward, regardless of the uncertainty in the absolute value. So either they are over reporting complicated cases (thus inflating estimated cases) or have tightened up their determination that a death is Covid related. The latter seems more probable, so they are probably now ruling out those who died with but not from COVID and only counting those who died from COVID. Mind you, this is just my best guess.
From this we can estimate that 25-50% of reported COVID deaths throughout 2022 and early 2023 may have been for other reasons.
The other trend to note was the upward number of complicated cases, which is why I eagerly awaited this weeks report and was bitterly disappointed it did not come.😢
Oh well, maybe its for the best. People seem happier, the masks are slowly but surely coming off more peoples faces, and besides the threat of drought, war, earthquakes, egg shortages, bird flu, future power terminations , food plant fires, enterovirus epidemic and typhoons, life is good.


