

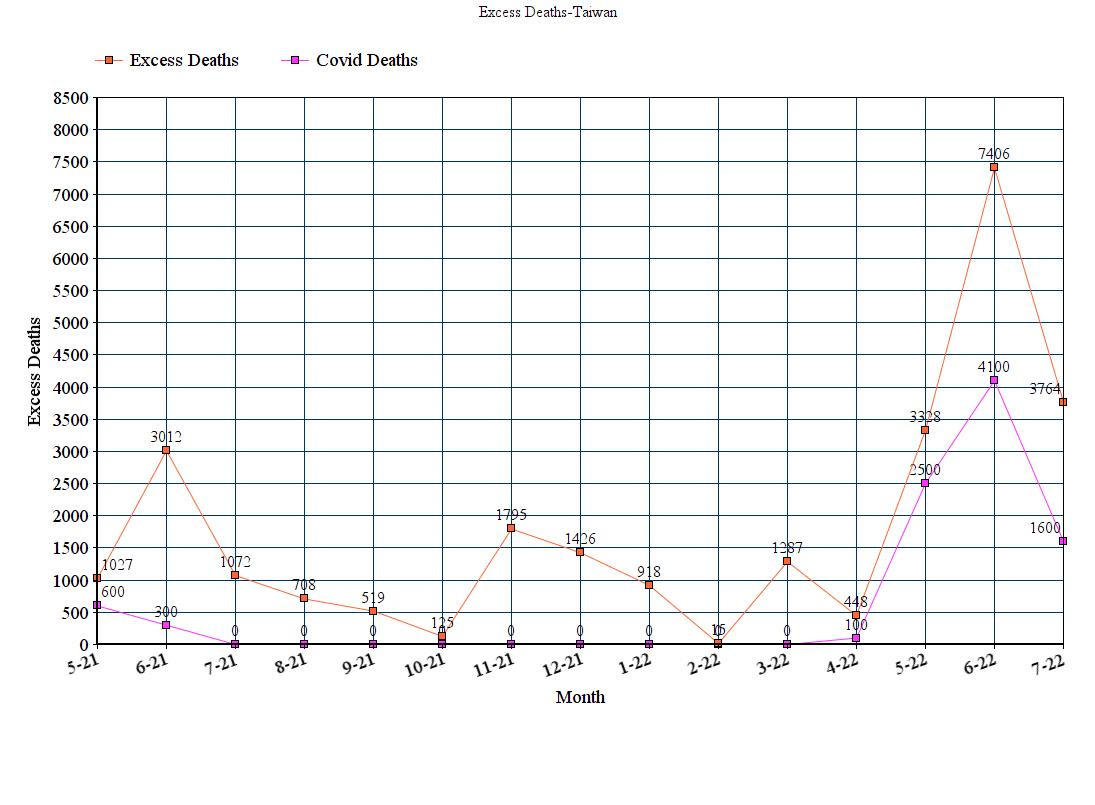
Excess Non-Covid Deaths, Taiwan

July Numbers of Total Deaths came out for Taiwan. I got to admit, they are efficient.
https://www.ris.gov.tw/app/en/2121?sn=22222422
So now for some Numbers
There were 241,222 total (all cause) deaths May 2021-July 2022. (13% more deaths than the 2016-2020 average hereafter referred to excess deaths)
Total Excess Deaths in the period
26, 842
From Worldometer and CDC Taiwan there were 9,273 COVID DEATHS as of August 9 with 9,262 COVID DEATHS occurring from May 1 2021 to Aug 9, 2022. This is only 35% of total excess deaths
Non-COVID excess Deaths since May 1 2021 is 17,580 which is 65% of excess deaths
As a control I looked at Excess Deaths from January 1,2020 to April 30, 2021 rule out a hidden wave of COVID prior to this period
Excess Deaths Jan 1 2020-April 30, 2021 was 873 (0.37% excess), this is not even close to being statistically significant. So no hidden COVID wave before May 2021
Vaccination began in April 2021 starting with the Elderly and HCW and Taiwans first COVID wave followed. Taiwans 2nd major wave began with Omicron Casedemic starting in January which was when the booster campaign began and cases increased gradually through April 14 with few deaths.
Booster Doses given
Jan- 5,500k
Feb -4,300k
March - 1,900k
April -2,100k
4th dose authorized for elderly in May (currently 31%)
May 1,400k
Jun 1,900k
July 1,100k

Purple is boost
After April 14 cases exploded with deaths piling up starting in May
Cases

Deaths

Its interesting but 98% of COVID deaths have occurred in May, June and July in both 2021 and 2022 (contrast with US where these months we see fewer COVID deaths). This is not true of excess deaths as 7241 (27%) of excess deaths occurred between August 2021 and April 2022
I cant explain the reason for the Excess Non-Covid Deaths. They all came after Vaccination and COVID waves began. There does not seem to be any clear correlation between deaths and booster doses administered in a given month and the majority of COVID deaths are in the Unboosted. I may look to try and stratify vaccine doses (all doses) administered by age if I have time and see if there is an association. The only proven association is excess deaths began after both the vaccination campaign and first COVID wave in 2021 and non-COVID deaths are higher during COVID waves.
If they are all COVID then somehow they are missing them. This seems more likely in the first wave in 2021 than in the second wave in 2022.
The COVID deaths are mostly in the Elderly (90%+ over 70’s) and unvaxxed make up 40-45% of the deaths in the second wave . This is far out of proportion to the unvaxxed population percentage of 8-10% but this may be due to the elderly are more likely to be unvaxxed

Many of the deaths are also in patients who have a DNR. So not just old

I cant find the age stratified data for the overall deaths to see if the Excess non-COVID deaths are occurring in a younger and more heavily Vaxxed population. Tis another mystery
One possibility might be a bias in determining cause of death. There is allegedly a committee that decides if a death is COVID or not. No idea if they have COI. It sometimes takes weeks or more to classify a COVID death and report it. I still see May or June Deaths being reported in July and August as a COVID DEATH.
For example here on 8/10 a death on 6/20 is confirmed as COVID on 8/8 (this case was boosted)

There may be a bias against classifying a younger and fully vaxxed person with few comorbidities as a COVID death. Or maybe not. I dunno.
Other considerations are the extensive use of Paxlovid starting in May. I believe up to 10% of the cases were being treated by June.
06/08/2022
The daily prescription rate of two oral COVID-19 antiviral drugs available in Taiwan exceeded 10 percent on Tuesday, Chen noted.
On Tuesday, a total of 11,427 courses of the two oral antiviral drugs were prescribed by doctors, including 9,102 courses of Paxlovid and 2,325 courses of molnupiravir, according to CECC data.
So far this year, Taiwan has used 130,504 courses of Paxlovid and 31,871 courses of molnupiravir, according to the data.
https://focustaiwan.tw/society/202206080023
Curiously based on my calculations (assuming they are right) the CFR for June cases was significantly higher than cases detected before June (0.21% vs 0.16% in May and 0.12% in January-April). This might be due to the higher volume of patients🤔
Why so many deaths in May, June and July which are some of the hottest month (someone is probably going to blame Climate Change). Outdoor masking mandates began in May 2021. Temperatures regularly hit 36-38 C here. Wearing a mask is hard in these temperatures especially for the elderly.
I cant say this would account for a large number of deaths but its something that should be looked at. I have seen virtually no long term safety studies on older and sick people wearing masks under such conditions
Obviously, during the lockdowns in 2021 and the constant stress of Pandemic hysteria over 15 months this affects peoples mental health and physical health in a way that may lead to more deaths
And lastly, one must consider the vaccines. But there is no way for us to do so in any conclusive fashion. Officially they are “safe and effective”.
Anecdotally I don’t hear a lot of talk about vaccine safety concerns. I think people who have them keep it to themselves. There was a bit of a scare among the elderly with the roll out last year which was with Astra Zeneca. This had a residual effect which is a reason the elderly have a lower vax rate than the younger people although the Omicron fear mongering and restrictions on the Unvaxxed that started in April boosted vax uptake.

Primary

One further observation on CFR. Obviously this can be distorted by the amount of testing done on mild/asymptomatic persons. In the first wave there was very little testing outside hospitals (in part due to draconian quarantine policies in which those who tested positive were removed from their homes and sent to quarantine hotels they had to pay for). In the first wave the CFR was 4-5%
The other extreme was noted in the second wave. Quarantine rules were relaxed (shorter and at home), rapid tests were made available for testing which would then be accepted as confirmation of being positive.
Here was the quarantine rules as of 5/22
B. Enhanced government quarantine facilities/quarantine hotels: asymptomatic/mild cases who are 70 years of age and older, who aged 65-69 and live alone, who are 36 weeks pregnant or more, who are 3-12 months old and have a fever over 39ºC, or who don't require hospitalization and don't meet home care criteria are all admitted to enhanced government quarantine facilities/quarantine hotels.
C. Home care: individuals with no/mild symptoms who are under 69 years of age and meet home care criteria may stay at home to receive care. Confirmed cases with no or mild symptoms who don't meet home care criteria can be allowed to receive care at home if confirmed cases themselves or their legal representatives request home care and after medical professionals' assessments.
https://www.cdc.gov.tw/En/Bulletin/Detail/YYvMotpITP0pMEPUaPmz9w?typeid=158
Plus many had taken out COVID insurance which paid out with proof of being a confirmed positive and the labour laws here provide for paid sick leave (50% of salary). No doubt the CFR in 2nd wave is closer to IFR and has ranged from 0.12 in April and 0.21% in June (by my calculations)
Taipei, July 31 (CNA) The top 12 sellers of COVID-related insurance policies in Taiwan have paid out nearly NT$32 billion (US$1.07 billion) in 2022, and the industry is set for a reckoning amid disputes over claims and payments, according to an expert in the protection of consumers' rights.
Low premiums of a few hundred dollars led to sales of millions of COVID-related infectious disease policies, but subsequent disputes created by a surge of cases beginning in April have exposed insurance companies' poor capacity for risk assessment, Consumers' Foundation Secretary-General Hsu Tse-yu (徐則鈺) told CNA in a recent interview.
https://focustaiwan.tw/business/202207310010
Age Distribution
So lets look at the age distribution of cases. All I could find was from May 26. Since nothing much changed we can assume the distribution has not changed much

As of May 26
Age. Cases %. Pop%
0-9 179,927. 11%. 9%
10+ 152,792. 9%. 9%
20+ 280,481. 17%. 13%
30+ 304,418. 19%. 14%
40+ 273,309. 17%. 16%
50+ 185,926. 12%. 15%
60+ 147,116. 9%. 13%
70+ 63,792. 4%. 7.3%
80+ 25,565. 1.6%. 3%
90+ 6,565. 0.4%. 0.7%
Total 1,612,891 cases as of May 26
Clearly the elderly (70+) are underrepresented case wise (6% of cases, almost 11% of population). Is this because they are being infected at lower rates (remember most transmission occurs within household) or a reluctance to test and report results for fear of being disappeared to a hospital. My wife and I are elderly. I suspect its the latter
BTW the CFR in the screen shot is too low. Thats because many of the cases from May /April had not died yet. My calculations since show the CFR was 0.12% before May and 0.16% in May. It jumped to 0.21% in June as cases started declining.
Was the case decline due to less infections (Farrs Law kicking in) or less reporting of positive results? Only the latter could have affected CFR. Of course, as I alluded above outcomes might have worsened due to either Paxlovid or hospitals being overloaded. We don’t really have good safety data on Paxlovid and unlike the vaccines there is no VAERS. Yet another mystery.
HOSPITAL CFR
What I would really like to see is hospital CFR (cases treated in hospital) but this is not being reported in Taiwan (at least not that I can see )
In US
In-hospital mortality fell from about 12% with delta cases to 7% with omicron.
https://www.npr.org/sections/health-shots/2022/01/29/1075871661/omicron-symptoms-treatment-hospital
From this table I might be able to estimate it

12,073 is the number of cases since January 1 with moderate symptoms
9,761 is the number of cases with serious symptoms
From my review of CDC daily death reports approximately 20% of deaths seem to have died at home, DOA or died on first day at hospital. If I exclude them we have 6,800 COVID deaths in hospital treated for 1 or more days
Assumptions
No asymptomatic/mild cases were being treated at hospital for COVID (elderly with Asymptomatic /mild symptoms were admitted after testing positive but its not clear if they were treated with Remdesivir or not which could result in deaths which would go down as COVID deaths)
All COVID deaths are in symptomatic COVID cases
All symptomatic cases were treated in hospital (unlikely to be true so this may result in a lower than actual hospital CFR)
Result
6,800 deaths/21,834 symptomatic cases=
31.14%. Lets call it 30%
That seems high to me since Hospital CFR for Omicron should be not much higher than 10%. I really would like to see the actual numbers. So assuming the number is much lower due to a faulty Assumptions (#1 & #2) this suggests patients may have died with COVID (or just a positive test w/o symptoms) but not necessarily due to COVID. However, without more data I can’t even guess
Still, even with a hospital CFR of 7-12% in US I cant understand the reluctance to try safe repurposed drugs. The only treatment protocol I could find for Taiwan was dated 2020 and I believe they still follow WHO/NIH protocols which say drugs like IVM not recommended outside a clinical trial.
Taiwanese experts on Monday warned against regular use of the drug in COVID-19 treatment, citing a lack of solid evidence.
“Following an experts’ meeting, we do not recommend regular use of ivermectin in treating COVID-19 due to the lack of enough evidence,” said Chang Shan-chwen (張上淳), convener of the Central Epidemic Command Center’s (CECC) expert advisory panel.
Chang said that no meaningful evidence has been provided to verify that it helps bring down patients’ mortality or intubation rate.
Neither is there evidence to prove that it speeds up the elimination of the coronavirus or shortens the length of a patient’s hospital stay, because of the limited number of cases studied, he said.
As neither the WHO, the EU or the US have included ivermectin use in their guidelines for COVID-19 treatment, the center decided not to recommend regular use of the drug for such a purpose, Chang said.
https://www.taipeitimes.com/News/taiwan/archives/2021/06/16/2003759259
Taiwan has a centralized medical system so it should not have been hard to put together a trial especially since they had plenty of time between the 1st and 2nd waves. Maybe they did and I just didn’t hear-about. If not, why?
I’ll end this here since I am starting to ramble.
Below is just the monthly death data I pulled from the pdf’s from the site linked above, but you can ignore without peril.
——————————————————
All Cause Death Data
Total Deaths-Jan 1 2020-April 30, 2021
235,058
Jan
2022-15,954 (+ 918)
2021-16,332 (+1,294)
2020-14,673
2019-16,622
2018-16,761
2017-12,835
2016 14,292
2016-2020 Avg 15,036
Feb
2022-14,887 (+15)
2021-14,856 (-16)
2020-16,211
2019-13,352
2018-14,493
2017-14,865
2016 -15,441
2016-2020 Avg 14,872
March
2022-18,239 (+ 1,287)
2021-16,438 (-514)
2020-16,083
2019-15,171
2018-17,200
2017-17,391
2016 -18,918
2016-2020 Avg 16,952
April
2022-14,655 (+448)
2021-14,276 (+99)
2020-14,423
2019-14,996
2018-13,988
2017- 13,110
2016 -14,520
2016-2020 Avg 14,207
May
2022-17,409 (+3328)
2021-15,108 (+1,027)
2020-13,272
2019-14,655
2018-14,328
2017-13,914
2016 -14,238
2016-2020 Avg 14,081
June
2022-21,033 (+7,406)
2021-16,639 (+ 3,012)
2020-13,893
2019-13,302
2018-13,043
2017-14,453
2016 -13,445
2016-2020 Avg 13,627
July
2022 18,215 (+3,764)
2021-15,523 (+1,072)
2020-14,533
2019-15,854
2018-14,372
2017-14,479
2016 -13,021
2016-2020 Avg 14,451
Aug
2022-
2021-14,952 (+708)
2020-13,301
2019-13,983
2018-14,162
2017-15,580
2016 -14,195
2016-2020 Avg 14,244
Sep
2022-
2021-13,894 (+519)
2020-13,876
2019-13,866
2018-12,866
2017-13,436
2016 -12,829
2016-2020 Avg 13,375
Oct
2022-
2021-14,415 (+125)
2020-13,542
2019-15,350
2018-14,922
2017-13,710
2016 -13,676
2016-2020 Avg 14,240
Nov
2022-
2021-15,560 (+1,795)
2020-14.141
2019-13,739
2018-13,680
2017-13,632
2016 -13,633
2016-2020 Avg 13,765
Dec
2022-
2021-15,739 (+1,426)
2020-15,208
2019-15,406
2018-12,949
2017-13,837
2016 -14 ,167
2016-2020 Avg 14,313
All cause
2022
Jan-15,954
Feb-14,887
Mar-18,239
April-14,655
May-17,409
June-21,033
July-18,215
Aug-
Sep-
Oct-
Nov
Dec-
119,392 thru July
101,177 thru June
2021
Jan-16,332
Feb-14,856
Mar-16,438
April-14,276
May-15,108
June-16,639
July-15,523
Aug-14,952
Sep 13,894
Oct-14,415
Nov-15,560
Dec-15,739
Full
183,732
2020
Jan-14,673
Feb-16,211
Mar-16,083
April-14,423
May 13.272
June-13,893
July-14,533
Aug 13.301
Sep-13,876
Oct-13,542
Nov 14.141
Dec-15,208
Full
173,156
2019
Jan-16,622
Feb-13,352
Mar 15,171
April 14,996
May-14,655
June-13,302
July-15,854
Aug-13,983
Sep-13,866
Oct-15,350
Nov-13,739
Dec-15,406
Full
176,296
2018
Jan 16,761
Feb 14,493
Mar 17,200
April-13,988
May-14,328
June 13,043
July-14,372
Aug 14,162
Sep 12,866
Oct-14,922
Nov 13,680
Dec 12,949
Full
172,764
2017
Jan-12,835
Feb-14,865
Mar-17,391
April-13,110
May-13,914
June 14,453
July 14,479
Aug 15,580
Sep-13,436
Oct-13,710
Nov 13,632
Dec 13,837
Full
171,242
2016-
Jan 14,292
Feb 15,441
Mar 18,918
April-14,520
May-14,238
June-13,445
July 13,021
Aug-14.195
Sep 12,829
Oct-13,676
Nov 13,633
Dec 14 ,167
Full
172,375
Full
2021 -183,732 (10,566)
2020-173,156
2019-176,296
2018-172,764
2017-171,242
2016-172-375
2016-2020 avg 173,166